In pharmaceutical manufacturing, cleaning is a validated, audited and documented act - not a chore. Pharmaceutical cleaning services sit at the very heart of GMP compliance, from cleanroom housekeeping to the validation of multi-product reactors. This guide details the standards, the MAC calculation, the sampling methods and the operator protocols that distinguish compliant plants from at-risk ones, with a focus on African facilities supplying local and export markets.
Key takeaways
- Pharmaceutical cleaning is a GMP discipline: every step is validated, documented and audited. WHO TRS, EU GMP, FDA cGMP and PIC/S all converge on the same expectations.
- Cleanroom grades (ISO 14644 A to D, EU GMP A to D) define particle limits, gowning, materials and cleaning frequency. The cleaning agent and the wiping technique change with the grade.
- Cleaning validation rests on three acceptance limits (visual, 10 ppm and pharmacological based on ADE/PDE), proven by swab and rinse sampling, with worst-case product selection and recovery studies.
- Operator behaviour - gowning, wiping technique, sequence - is the single most common cause of validation failure. Training, qualification and routine surveillance close the loop.
Why pharmaceutical cleaning is its own discipline
Cleaning a pharmaceutical plant is structurally different from cleaning a food line or a refinery, even though the three appear in the same broader industrial cleaning services catalogue. The difference comes from three factors. First, the patient safety stake: any residue carried into the next batch can be ingested, injected or inhaled by a vulnerable person. Second, the multi-product reality: most African pharma plants run several APIs on the same equipment, generating cross-contamination risk by design. Third, the regulatory weight: every cleaning protocol is validated, qualified, periodically reviewed and audited by national and international inspectors.
The GMP regulatory framework
Global references
Four global frameworks shape the practice. WHO TRS Annex 4 and 5 define the GMP for medicinal products in WHO member states. EU GMP (Eudralex Volume 4) governs European market access, while FDA cGMP (21 CFR 210/211) governs US imports. PIC/S harmonises these expectations across more than 50 regulators. Every contract manufacturer exporting from Africa to regulated markets must demonstrate compliance with at least one of these.
African regulators
At national level, NAFDAC in Nigeria, the Food and Drugs Authority in Ghana, the Pharmacy and Poisons Board in Kenya and SAHPRA in South Africa enforce GMP inspections, issue manufacturing authorisations and can suspend production permits. The African Medicines Agency (AMA), now operational, is gradually harmonising standards across the continent.
Cleanroom standards: ISO 14644 and EU GMP grades
Pharmaceutical cleanrooms are classified by the maximum allowed concentration of airborne particles. ISO 14644-1 defines classes 1 to 9, while EU GMP and WHO use grades A to D. The two systems intersect: Grade A roughly maps to ISO 5, Grade B to ISO 5 (at rest) or ISO 7 (in operation), Grade C to ISO 7 / ISO 8, Grade D to ISO 8.
| Grade (EU GMP) |
Typical use |
ISO equivalent (operational) |
Cleaning frequency |
| A |
Aseptic filling, critical operations |
ISO 5 |
Pre/post each operation + daily deep clean |
| B |
Background for Grade A |
ISO 7 |
At each shift + weekly deep clean |
| C |
Solution preparation, weighing |
ISO 8 |
Daily |
| D |
Less critical activities, packaging |
ISO 8 at rest |
Daily |
Cleaning validation: MAC, ADE and worst case
The three acceptance criteria
Cleaning validation establishes that residues left after cleaning are below safe limits. Three acceptance criteria are combined: visual cleanliness (no residue visible to the naked eye, typically below 4 micrograms per square centimetre), the 10 ppm criterion (no more than 10 mg of previous product in the maximum daily dose of the next), and the pharmacological criterion based on the Acceptable Daily Exposure (ADE) or Permitted Daily Exposure (PDE) calculated from toxicological data. The Maximum Allowable Carryover (MAC) is then converted into a surface residue limit per square centimetre.
Worst-case product selection
Validation does not test every product combination. A worst-case product is selected on the basis of solubility, hardest-to-clean nature and lowest ADE/PDE. Demonstrating that this worst-case product is cleaned below acceptance limits validates the entire matrix.
Sampling methods: swab versus rinse
The two sampling techniques recognised by all GMP authorities are direct (swab) and indirect (rinse). They are complementary, not interchangeable.
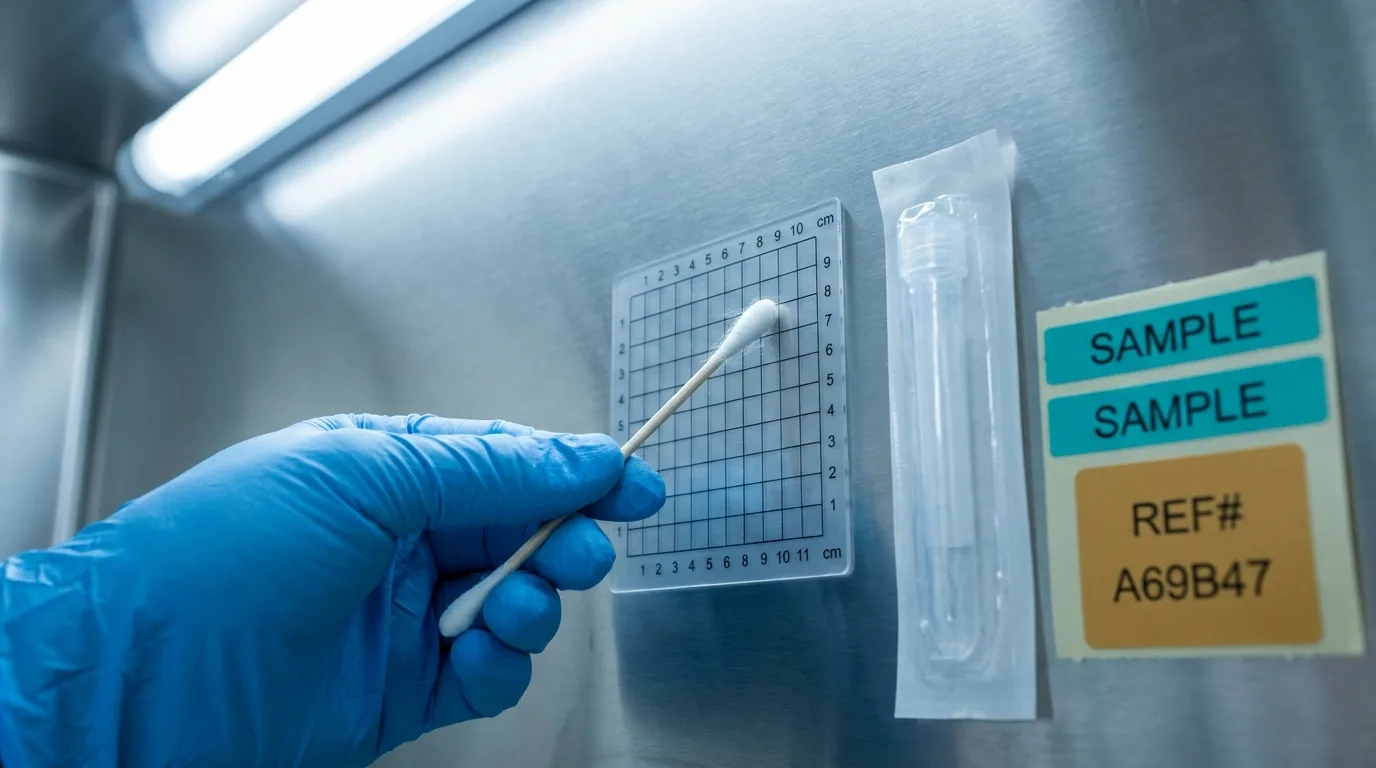
Swab sampling on a defined template is the gold standard for cleaning validation in pharma.
Swab sampling tests a defined 5x5 cm or 10x10 cm area on a precise surface, typically the hardest-to-clean point of the equipment (T-bends, mixer blades, sample valves). Rinse sampling collects the final rinse water and tests it by HPLC, TOC or specific assay. The recovery rate of each method must be qualified during validation through known spike-recovery studies.
Cleaning agents in pharma
Pharma cleaning agents are usually limited to a short, validated list: water for injection (WFI) or purified water, neutral or alkaline detergents (typically 0.1 to 2% concentration), occasional acid cleaners for mineral deposits, and sanitizers (70% IPA, hydrogen peroxide, peracetic acid) for environmental surfaces. All must be supplier-qualified, pharmaceutical grade where applicable, and supported by a complete documentation pack (MSDS, certificate of analysis, residue data). The broader chemistry behind these choices is covered in our industrial chemical cleaning guide.
Gowning, training and operator behaviour
The single biggest source of cleaning validation failure is operator behaviour: wrong wiping direction, insufficient contact time, contaminated wipes, gloves touched on the outside, sequence skipped. Gowning qualification, three-cycle dressing audits, on-the-job retraining and routine glove monitoring are the levers that GMP-compliant plants use to keep failures at the floor under 1%.

Gowning vestibules are designed to prevent particle and microbial ingress between cleanroom grades.
Wiping techniques that pass validation
-
Top to bottom: clean the top of the equipment first, allow gravity to take the residue down.
-
Clean to dirty: never go back from a soiled wipe to a clean area.
-
One direction, overlapping passes: never zig-zag, always overlap by 25% to ensure full coverage.
-
Fold and rotate: each wipe has four to eight clean surfaces; the operator folds and rotates between passes.
-
Replace at the first sign of dirt: a soiled wipe redistributes contamination.
Cleaning frequencies and the master cleaning plan
A pharma master cleaning plan combines three layers. Routine cleaning happens at every product changeover (campaign cleaning), at the end of every shift, and on a fixed daily schedule for environmental surfaces. Deep cleaning addresses ceilings, return grilles, behind-equipment voids on a weekly to monthly basis. Periodic cleaning of HVAC HEPA filters, pipework and storage areas is scheduled quarterly to yearly. Every cleaning is documented and electronically signed by the operator and the supervisor.
Sustainability in pharma cleaning
Water for injection and purified water carry a very high embedded cost (energy, filtration, distribution). Strategies to recycle final rinse water for non-critical uses, reduce IPA consumption, switch to single-step combined detergent-sanitizers and source pre-saturated wipes locally are now standard ESG levers - explored in detail in our companion piece on sustainable industrial cleaning .
Frequently asked questions
How often is cleaning validation re-confirmed?
Cleaning validation is initially done on three consecutive successful runs. Re-validation is triggered by any change (new product, new equipment, new detergent, modified process) and otherwise on a periodic basis defined in the validation master plan, typically every 2 to 3 years.
Is dedicated equipment required for high-potency APIs?
For most high-potency or cytotoxic APIs, regulators require either dedicated equipment or, when shared equipment is unavoidable, a documented Health Based Exposure Limit (HBEL) demonstrating that residues remain below safe levels. Engineering controls (isolators, closed transfers) are usually mandatory.
Can we use the same detergent for all equipment?
Yes, provided every product and surface combination is covered by validated worst-case studies. Many African pharma plants standardise on one alkaline detergent and one acid cleaner to simplify validation and procurement.
What documentation must support a pharma cleaning operation?
Standard documentation includes the cleaning SOP, the operator training and gowning qualification records, the batch cleaning record with electronic signatures, the routine analytical results (swab, rinse, environmental monitoring), and the periodic review report. Inspectors expect to retrieve any record within minutes during an audit.
How do I choose a contractor for pharmaceutical cleaning?
Look for GMP-trained operators, valid gowning qualifications, hands-on experience in your therapeutic area, capacity to produce validated cleaning protocols and SOPs, and a documented training matrix. The industrial cleaning services pillar guide details the wider selection checklist that applies on top of these pharma-specific criteria.



















































